[00:00:04] Speaker A: ID the Future, a podcast about evolution and intelligent design.
[00:00:12] Speaker B: Welcome to ID the Future. I'm your host, Eric Anderson, and I'm pleased to be joined again today by Dr. Howard Glicksman to continue our discussion about the many challenges life has to overcome in order to continue to survive. Dr. Glicksman practices palliative medicine and is co author of the recent book your Designed Body. Welcome, Howard.
[00:00:30] Speaker A: Thanks, Eric. It's great to be back.
[00:00:32] Speaker B: So last time we challenged the notion that the natural result of physics, even as wonderful and as fine tuned as physics may be, would lead to living organisms. In fact, we saw that the natural result of physics and chemistry left to their own devices is to cause death, not life. So for those who might just be joining us, Howard, maybe very briefly explain what you mean by that, and then I'd like to dive into a few more details.
[00:00:57] Speaker A: Yeah, so what I'm basically saying is that the idea of Darwinism is basic, is that to say that the laws of nature on their own, left to their own devices, can cause life, but with how we know, we know that they actually cause death. And what we talked about last time was we looked at two laws of nature, diffusion and osmosis. We looked at it at the cell level because we looked at the water and its solute. So the cell has water inside it and it has high potassium, low sodium, and high protein, whereas the water outside the cell has high sodium, low potassium, and low protein. So diffusion and osmosis, when left to their own devices, are going to cause the sodium and the water to enter the cell and the potassium to go out. And when that happens, it causes death. And the innovation that life has to come up with to solve this problem is, is something called the sodium potassium pump. And you have about a million of them in each of your cells. And at rest, they use up about 1/4, maybe to 1 half of the energy your body uses just to keep those cells growing together. So basically, the laws of nature cause death unless life comes up with innovations to combat it or use it to its advantage. Or in other words, solve these hard engineering problems that the laws of nature throw at life.
[00:02:16] Speaker B: Yeah, and I'd encourage anybody who didn't catch it. Go back and listen to our prior episode. Very interesting how the sodium potassium pump helps to maintain the cells volume number one and chemical constituents number two. That's really great. So that's on the level of a single cell. Howard, what if we start a multicellular organism like ourselves? How does that play out?
[00:02:36] Speaker A: So what we. What I mentioned last time is to go through it again is that your body.
Your body has about 60% water, and two thirds of that water is inside your cells, and one third is outside your cells. It's called the extracellular fluid. But of that water, 80% is in the interstitial fluid. It's between your cells, and 20% is actually in your bloodstream. So when we start talking about a multicellular organism like us, we realize that we need a blood system to be able to pass on oxygen.
Are you hearing that?
[00:03:09] Speaker B: Oh, yeah. What's going on? What's going on there?
[00:03:12] Speaker A: Yeah, we're down in Florida here. It's that time of day.
[00:03:14] Speaker B: You're getting thunderclaps.
[00:03:15] Speaker A: Yeah, just hearing some thunderclaps.
[00:03:18] Speaker B: Go ahead. We'll work through it here.
[00:03:20] Speaker A: Okay, so. So what we talked about. Two things to keep in mind that what we talked about last time was the sodium potassium pump is very important for keeping sodium out of the cell and water with it and making sure potassium stays inside the cell. So at one level, not only the sodium potassium pump also makes sure that there's enough water in the extracellular fluid. So without the sodium potassium pump, you wouldn't even have enough fluid in your bloodstream. But here's the key thing. The. The way your body works is the interstitial fluid acts as a bridge between your cells and your intravascular fluid. So if you have oxygen or sugar coming in, comes into the bloodstream, comes down to the capillaries, and then it moves by diffusion into the interstitial fluid, and from there, it goes into your cells. Okay. And carbon dioxide from inside the cell goes out, out into the interstitial fluid and goes into the capillary into vascular fluid. So diffusion, when you're talking about the circulation, diffusion is really good for, say, oxygen, carbon dioxide, because the carbon dioxide can transfer from the cell to interstitial fluid to the intravascular fluid, and oxygen can go the other way. Right?
[00:04:30] Speaker B: Yeah.
[00:04:31] Speaker A: And osmosis is very good, too. So water moves in your body by osmosis. So very important to understand that during the day, you're always losing water from sweating, from urine formation, from breathing. You lose water vapor there in the GI system. So your body's always losing water. And that water comes out of the extracellular fluid. So it's coming out of your intravascular volume, and it's also coming out of your extracellular fluid. So when that happens, when the water starts coming out of the extracellular fluid, that makes the chemical content inside the concentration go up. And so the water Moves from inside the cell to cross over to make up for that. So this is why, although your body can't store oxygen, you can only live three or four minutes without oxygen. Your body can actually store water. There's only so much water that the cells can give up. But if you go several hours or working hard, that's how the cells can transport water over. And then when you drink water, the water goes into the GI system, gets absorbed into your intravascular volume, it goes into your extracellular fluid, it dilutes that, and therefore the water then trans. Then that becomes more dilute than inside the cell. So the water by osmosis then goes inside the cell.
[00:05:40] Speaker B: So, okay, so hang on a second. Hang on a second. Thought through a lot there.
So let's talk about dehydration for a second. So I haven't been drinking enough. The water volume in my bloodstream goes down. The water volume in the interstitial fluid goes down, and the water volume now in the cells starts compensate. So I'm literally pulling water out of the cells by osmosis to help put more water into the interstitial fluid and into the bloodstream. Right. So my cells are literally shrinking. Is that what's going on at that point?
[00:06:13] Speaker A: Exactly. But. But also the point. I love the way you put that, because this is an example of how life can leverage the laws of nature. Because when you're active, right, because of osmosis, you've got this storage or water, and the water can buttress the fluid in the intravascular volume. Because if you go too low, if you get dehydrated, then what happens is not only does the cell shrink too much and it's got its own problems, but you lose intravascular volume. So then your blood pressure drops, your blood flow drops, and you die. I mean, this is how you go into shock. So if you get. If you lose too much water from the body, the body can maybe lose 20 or 25% of its water, and then. And then you die because the blood pressure drops too low and the cells got too small. So.
[00:06:53] Speaker B: Yeah, and this is why we have a reminder on our phone that says, drink something every hour. Right. Or is there another way that the body reminds us?
[00:07:01] Speaker A: Well, okay, yes. Okay, so. So. So you actually have these.
[00:07:05] Speaker B: I just pass out all the time, Howard. I forget to drink for, you know, a couple of days and just die on the street.
[00:07:09] Speaker A: Right, well, that's a good point, because certain. Certain neurological injuries can get rid of the thirst center. So when you actually have. Technically, you have shrink sensitive cells in your hypothalamus that detect that your body is losing water and it sends a message to your thirst center. That's the reason. That's one of the reasons that tells you to drink water. Okay. That's part of the reason why. There's other reasons. There's other things that trigger the thirst.
[00:07:32] Speaker B: Yeah, Let me make sure everybody catches that though, because that's pretty impressive. So you're saying there's specific cells that. In the hypothalamus, did you say?
[00:07:40] Speaker A: Yes, they're in the hypothalamus. Yeah.
[00:07:42] Speaker B: Okay, so we've got the hypothalamus in your brain that has specific cells that can detect that they're shrinking.
[00:07:49] Speaker A: Yeah, they're actual shrink sensitive cells. They actually, when the cells shrink, they send a nerve message to the thirst center that's also in the hypothalamus telling you to drink. It also sends a message to another hormone system which.
[00:08:03] Speaker B: Yeah, there's a lot. I know there's a lot going on.
[00:08:04] Speaker A: Yeah, there's a lot going on which we'll leave it. We won't go there.
[00:08:07] Speaker B: I just want to point out there are cells that actually have sensors that detect when the cells have shrunk too much and are calling for the body to get more water in. Right?
[00:08:18] Speaker A: Yes.
[00:08:18] Speaker B: Plus other things dealing with the sodium, potassium.
[00:08:22] Speaker A: So last time we talked about osmosis, right? Osmosis is when, remember we talked about with the water moving from the cell to the intravascular volume because intravascular fluid, because you're losing water and the chemical concentration goes up. Well, it's actually the osmotic.
The osmotic.
I guess it's the osmotic power in there goes up because the concentration goes up. Well, these cells are called osmoreceptors.
So it's because what's going on is not only the cell shrinking, but the fluid inside the cell, the chemical concentration in that cell is going up too. It's reflective of everything else in the body because, see, the water shifts back and forth.
[00:09:02] Speaker B: Okay, that's very interesting. So do we know yet whether the sensors are detecting osmotic pressure or whether they're detecting size or detecting concentration? Do we know what they're sensing?
[00:09:14] Speaker A: It's a good question. I think the idea is that they're shrink sensitive. So I think they go by the size of the cell.
Yeah, I think it's a good question because, you know, who knows, 20, 30 years from now we're going to find out.
[00:09:26] Speaker B: It's probably both Good research project for young people out there.
[00:09:29] Speaker A: Yes. Is it just osmo, is it able to actually detect the actual chemical concentration? But the thing is, is that the, the, the shrinking of the cell is sort of an indirect measure of that. It's like a surrogate, surrogate marker for having increased osmolarity, higher concentration of chemicals because that, that correlates with the cell shrinking.
[00:09:52] Speaker B: Yeah, sure. Okay, so, so, so go ahead.
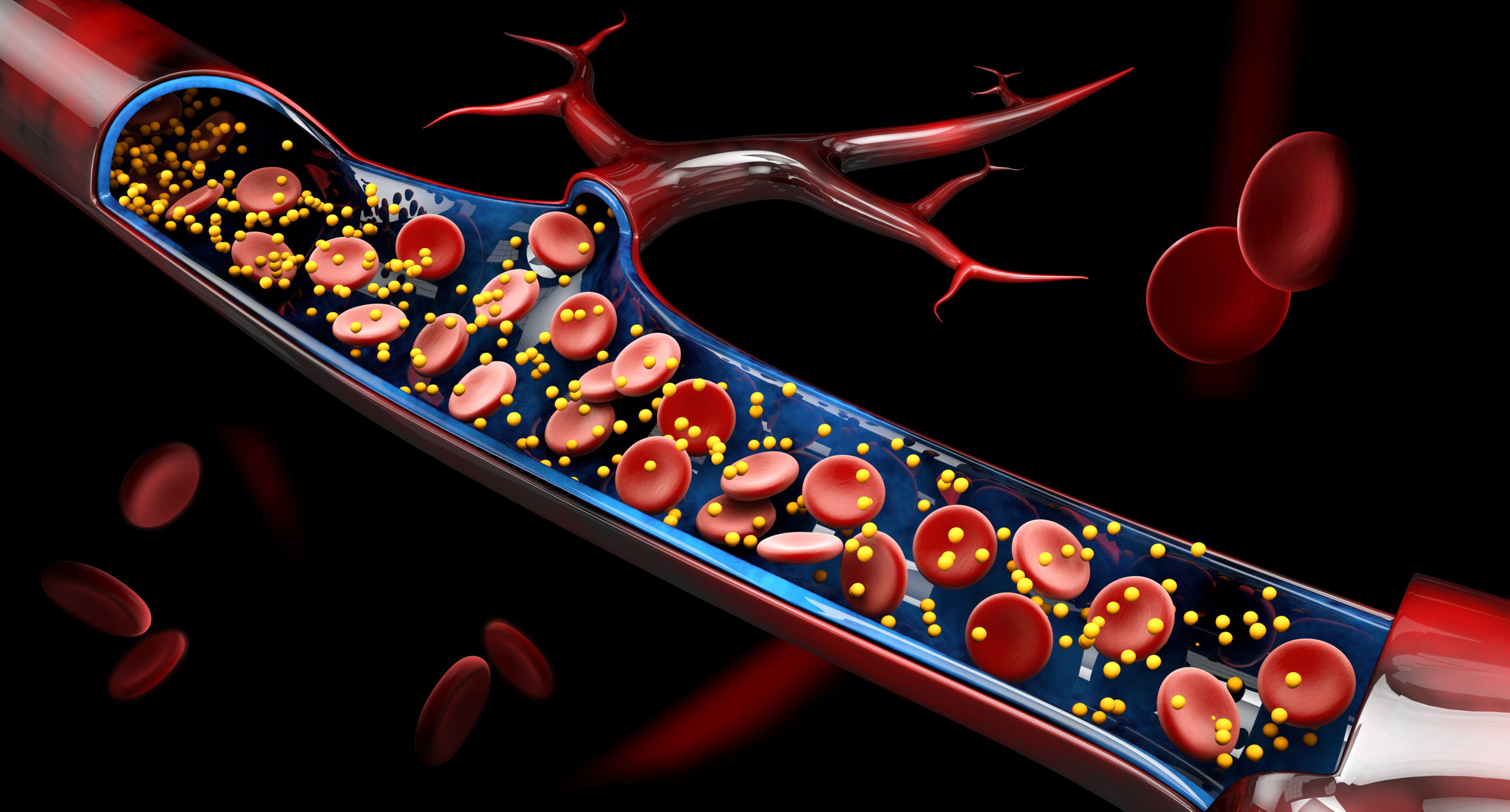
[00:09:56] Speaker A: Okay, that's a good question. It's a good, you know, segue to. We'll get into what, what I wanted to talk about today, and that is what's very important. So now we're going to look at how the laws of nature, how they can affect the cardiovascular system at the level of the capillary. So we have to look at how the body provides water and its chemicals to the cells. And we know that the heart pumps blood, hearts, blood from the left heart, left ventricle, goes up through the main arteries, comes down through the arterioles, and then the blood goes into the capillaries. Now it's important to know that at the level of the heart, the mean arterial pressure, people are used to like 120 over 80, 130 over 70, whatever. But there's a way of determining a mean arterial pressure is about 100 millimeters of mercury. Okay. But by the time the blood gets all the way down into the arterioles, and don't forget, along the way, kinetic energy is being used up, so the power is being lost. And also you've got muscles around the arterioles that are sort of slowing down the blood to get in there. And by the time it gets to the capillary, it's about 35 millimeters of mercury. Now I liken this to electricity coming into your home. If the electricity at the power plant, if it came out and it came straight into your home, it would blow out all your appliances, blow everything up. So you've got the step down transformers, et cetera. So by the time the electricity comes into your home, it's at a level that your appliances can handle it. It's the same thing here. If the blood came in as your capillaries at 100 millimeters of mercury would just blow the capillaries out. All the water, all the water in your blood would just be pushed into the interstitial fluid. It's just too fast, too hard, right?
[00:11:34] Speaker B: Okay, so, so for those of us who don't deal every day in millimeters of mercury, we, we like things like pounds per square inch more than millimeters of mercury. But the point is it's 100 in the arterial system and 35 by the time it gets through the, the small arteries, right?
[00:11:53] Speaker A: By the time it gets to the arterial end of the capillaries, as it starts to come into the capillary, that's.
[00:11:58] Speaker B: A pretty big drop from 100 to 35. That's what we'll keep in mind is.
[00:12:01] Speaker A: Down, down at 35. So now, now what happens is that that blood gets pushed with hydrostatic pressure through the capillary. Then the capillary walls are leaky. So we know that chemicals like carbon, oxygen, and sugar will go, will diffuse through the capillary wall into the, into the interstitial fluid, but so will water. So, so you have this, what's called ultra filtration because technically the water is being pushed through, right? Some of, some of the water is being pushed through the capillary into the interstitial fluid. And so the problem is, is that even at 35 millimeters of mercury, that's a lot of water. I mean, what happens? Because we have to make sure. Remember I said the, the extracellular fluid. 80% is interstitial fluid, 20% is, is in the intravascular volume.
[00:12:47] Speaker B: Right?
[00:12:48] Speaker A: What happens if more and more water goes into interstitial fluid? You're going to reduce the amount of blood volume, which is going to drop your blood pressure, drop your blood flow, and you're going to die because you got not enough blood flow to your tissues. So here's an opportunity for the laws of nature. Ultra filtration, this hydrostatic pressure that's pushing the water through the capillary at 35 millimeters of mercury, that's too high. Too much water is going to go out. So you need a counterforce.
The body is set up with a counterforce to bring that water back. So, and what it is, is on osmotic pressures, what I neglected to mention here is in this interface, the interface between the interstitial fluid and the intravascular fluid is the capillary membrane, your capillary wall. And it happens just like in this situation. The blood, the blood's going through has a higher amount of protein because your cells make, excuse me, your liver makes a lot of protein because, you know, your body needs these proteins. And the, and the interstitial fluid has a low amount of protein. Okay, so once again, we're, we got the setup again where the fluid that's going through the capillary has a high amount of protein compared to the fluid outside. On the outside of the capillary of the interstitial fluid. And it happens that you have plasma proteins, but probably the most important one is something called albumin, sort of like the white of an egg. And it represents about it, it represents what it made in the liver. It's about 50% of all the protein that the liver makes.
But that plasma protein has a certain amount of osmotic power because it, remember, it's staying in the blood supply. So the water is going to be pulled back by that albumin. And they can actually calculate it. But in average, it's about 25 millimeters of mercury. So what ends up happening is as that blood goes through the capillary, it comes in at 35 millimeters of mercury.
The albumin, that's it. The plasma protein that's inside the capillary is pulling it back at 25 milliliters of mercury. So you've got a net filtration about 10 millimeters of mercury. By the time the blood goes through all the way to the end of the capillary, the hydrostatic pressure has lost power. It's down to about 18.
So now it's only 18 millimeters of mercury. But the osmotic power still stays at 25 along the way. And now at the other end of the venous end of the capillary, the water is being pulled back into the bloodstream at about 7 millimeters of mercury. So a certain amount of water is left in the interstitial fluid and that actually goes into your lymph vessels. This is what, you know, manages immune function.
[00:15:14] Speaker B: Okay. You've covered a lot there, in addition to the thunderclaps in the background.
[00:15:18] Speaker A: Yeah, sorry about that.
[00:15:19] Speaker B: Yeah. So let me see if I could sort of, for our listeners, recap here a little bit. So there's a type of garden hose that I've had before that you can buy that has like these little pores in it, and you lay it out on the, you know, on the ground and it sort of leaks out a little bit of water here and there. So that's one thing to think about with, with respect to the capillaries. They're kind of leaky as you use that term. Right. The other thing to remember and correct me if I'm wrong, this is a closed loop system. So unlike my garden hose that ends, you know, at the end of the run, it's actually a closed loop system. So it's coming back around. Correct, Right. Yeah. So what we have, if I'm understanding you right, is we have this desire of the water to be pushed out at 35 millimeters of Merc.
But we have albumin, this plasma protein that's remaining in that hose while it's going through, and that tends to pull the water back or prevent it from leaving, however you want to see that, but prevent the water from leaving or pull it back in. So we're now down 10 millimeters of mercury. Right. Which is. Which is more reasonable for what we need for the interstitial fluid and what we need to maintain our water volume in the. In the vascular system.
[00:16:29] Speaker A: Right, exactly.
[00:16:30] Speaker B: Then as that continues on and we get from the starting point of that capillary, now we're heading back to the heart.
Right. So we're now at the venous end. We're actually pulling in even more water. Right? Is that what you're saying? So we're pulling some of the water back into the system from the interstitial fluid, if I got that right.
[00:16:48] Speaker A: So. Yeah, so I think you put it very well, and I think. I think you put it better than I did. That basically, at the arterial end of the capillary, at Arteriola, into the capillary, it's a net. Instead of 35.
Yeah, 35. Minus 25. So there's a net filtration of 10 millimeters of mercury, which has made it reasonable. But by the time that that blood's gone through the other end, the capillary is pulling it back in, because now it's minus seven. Now the, The. The hydrostatic pressure is reduced enough so that the actual osmotic pool is stronger. And so now some of the water that's been pushed out into the interstitial fluid is now being brought back into the street and then from the venue at the other end, and that goes up through larger and larger veins back to the right side of the heart. So the reason why this is so important, and we know this is important in medicine, I mean, right now it's sort of an abstract sort of thing, is that the key thing is that the normal. The normal level of album in the bloodstream is three and a half. I'm not going to get to the units, but it's 3.5 to 5 units.
[00:17:47] Speaker B: Okay.
[00:17:49] Speaker A: And the problem is, the doctors will tell you if someone is not making enough albumin, there's many reasons why it can be low. Probably the commonest is liver disease, sometimes kidney disease. The proteins being lost in the bloodstream through the kidneys. I'm sorry, through the urine. The point here is that when the albumin level gets too low and that osmotic pull is reduced from 25, maybe down to 21 or 20, then more and more fluid is going to stay leak and stay in the interstitial fluid.
And when that happens, then people tend to get what we call edema where their legs swell up. This is what I deal with because I'm a hospice doctor. I deal with a lot of these people with heart failure and I help them get rid of the fluid if I can. And so when it gets down to like, instead of 3.5 to 5, if they're, if their level is like 1 1/2 to 2, then too much water is coming out of the, through the circulation into the interstitial fluid. And therefore their blood pressure tends to be low, their blood flow tends to be low. These people tend to be hypotensive. They can't stand up. And frankly, I've never seen it. My understanding is an albumin level, less than one unit is incompatible with life. Okay. Because probably at that level, I looked it up, but I couldn't find it at that level. The osmotic pull back is so low. Right. It's probably below 18, it's under 18. So that means the capillary is always leaking water through. Okay. So you're just, and this is very important, this is how the laws of nature, in this case, you're using hydrostatic pressure to ultra filtration. That works great to move fluid around and you know, to get to fill up the lymph system, et cetera. But you need the balance by the osmotic pull of albumin and plasma proteins to make sure you still have enough fluid in the intravascular space. And if you don't have that, and we know from the numbers, this is where the numbers are very important. If it gets below a certain level, we know that's incompatible with life. And so the question is, albumin consists of 585amino acids. How does the liver know how to make it? We're not even sure how the liver knows how much to make.
[00:19:50] Speaker B: Okay.
[00:19:50] Speaker A: And all those sort of things.
[00:19:52] Speaker B: Yeah.
[00:19:52] Speaker A: And that's, that's sort of where your next question. This is an example of how the laws of nature can cause light. It could cause death.
[00:20:00] Speaker B: Yeah. Left to their own devices, would kill you if life didn't come up with this innovation of albumin.
[00:20:05] Speaker A: Right.
[00:20:06] Speaker B: And the information needed to build it and how much to build and so on and so forth.
So by the way, am I, am I wrong in saying that part of your expertise is in body fluid levels is that part of what you do.
[00:20:18] Speaker A: Yeah. I have patients who often come on hospice with heart failure. And what they've got is.
Their problem is they've got a massive fluid overload problem. And I've been able to come up with some innovations of readjusting their medication.
That doesn't seem to be known out there by a lot of people, it seems, but a lot of times I'm able to readjust their medication and get rid of their fluid, sometimes discharge them from hospice alive or, or certainly make them a lot better. You know, take 20 or 30 pounds of fluid off and it's, it's, it's just understanding the situation.
[00:20:49] Speaker B: Yeah, it's very interesting because you say they come in diagnosed with heart disease. Right. Which is probably true. But the underlying problem is this managing of these liquids, the fluids that we've talked about over the last couple of times that we've talked, Howard, with osmosis and diffusion and sodium, potassium pumps and albumin and everything that.
The receptors, I forget what you call them, the osmotic receptors that tell you when you need to bring in more fluid, everything else that goes on with that. So there's a lot of underlying things that actually are going on that would contribute potentially this person's condition that you've been able to help them with. I think that's just fascinating. Yeah.
[00:21:29] Speaker A: Just very simply, what happens in these situations is. I told you about the osmoreceptors. Well, that turns on a hormone to make the body hold onto water. But also when this is happening, it also turns on hormones in the kidneys, hormones that affect the kidney to make it hold on to salt. So that's another.
I'd be happy to come back and talk about how all that works, how the body controls sodium and water, because they're two different systems. But they, but they overlap. And it's just fascinating. But that's. But this is a situation where they're counterproductive. The body thinks it's going into shock, so it turns on these systems and starts holding onto water and salt. That's what happens with these people with heart failure. Because the, the, in the heart situation, it's not pumping the blood well enough through the arterial system. It's called arterial under filling.
And so the body reacts as if it's in shock. It says, oh, we're not. There's not enough blood pushing through. The problem is not that it's in shock. It's not that it's getting dehydrated or bleeding. It's because the heart's not working. Right. But it reacts by turning on certain hormone systems that so. Because there's several things that control blood pressure and that I'd be happy to come back another time to go through it because it's just, it's just fascinating stuff. But, but because I think because of what I've done there, I think it's helped me to understand all this stuff that I write about intelligent design and explaining how all that works.
[00:22:46] Speaker B: Yeah, No, I appreciate it. Well, Howard, thank you so much for being with us to help us appreciate a little bit better what's actually involved in maintaining a living organism and some of the engineering challenges that have to be overcome. Just really deep design that's required to accomplish this herculean task. So thank you for being here.
[00:23:03] Speaker A: It's been a pleasure. Thanks a lot, Eric.
[00:23:05] Speaker B: So to get your copy of your designed body written by Howard Glitzman and Steve Laughburn, you can look at Amazon or other retailers. And thank you for listening to this episode of ID the Future. To learn more about the remarkable engineering of Live, please join us again at ID the Future on your podcast app of choice and help us reach more people with this important message by sharing a link with a friend. For ID the Future, I'm Eric Anderson. Thanks for listening.
[00:23:32] Speaker A: Visit
[email protected] and intelligentdesign.org this program program is copyright Discovery Institute and recorded by.
[00:23:40] Speaker B: Its center for Science and Culture.